
جوري
Soldier Through It!
- Messages
- 27,759
- Reaction score
- 6,095
- Gender
- Female
- Religion
- Islam
I don't know how many med students there are on board, or how useful this review will be for you.. I am a firm believer in slow and consistent than an intellectual enema two days before the exam where once released never again to be regained.. So what I plan to do here, is share some things I feel are important..
In my pre-clinical years, I was president of the pharmacology club, and I enjoyed teaching it and exchanging ideas with others.. so if you have your own forte, quirks mnemonics that you'd like to share we can make a useful compendium..
I am only going to focus here on pharmacology and diagnostic testings.. so every day I'll give you five of each..
I am not going to start in any particular order but once in a section, I plan to complete it.. this will be just the high yield..
_____________________________________________________________
Oncology diagnostic testing
_____________
AFP (what disease is associated with it, and when do you answer this for a question?)
AFP is associated with the development of
1-hepatocellular ca.
2-ovarian cancer
3-non-seminomatous germ cell tumors
Answer AFP when you see a patient with alcoholic cirrhosis or chronic hepatitis B or V. AFP together with radiological imaging is used to screen for hepatocellular ca
____________________________________________
CEA
1-A protein elevated in a variety of cancers including colorectal cancer
2-serum CEA have a prognostic value in pts with newely diagnosed CRC. Those with higher levels have worse prognosis.
3-CEA level to monitor in colon cancer in pts after a surgical resection, it determines the presence of persistent, recurrent or metastatic disease
_____________________________________________________________
Colposcopy
Colposcopy is the direct visualization of the cervix, by use of a magnifying scope with a lamp
2-The transition zone must be visualized to ensure an adequate colposcopy. The border between squamous and columnar epithelium
3-a colposcopy is the answer for a pt with an abnromal pap
Atypical squams can't exclude high grade lesion ASC-II
low grade squamous intraepithelial lesions LSIL
high grade intraepithelial lesions HSIL
Atypical sqams of undetermined significance ASCUS if HPV DNA testing is positive
_____________________________________________________________
Estrogen and progesterone receptors
Should be done on all pts with breast cancer, in order to determine who should receive hormone therapy
2-Therapy with either tamoxifen or raloxifene should be added to any pt. with positive receptors. This is either for estrogen or progesterone positivity alone or in combination. The response to tamoxifen is better if both receptors are positive
______________________________________________________
Mammogram
screening should begin at age 40 and should be performed every 1~2 years, screening at age 50 should be yearly
2-when mammogram shows abnormalities, a core biopsy including sentinel lymph node biopsy is the next best step. carcinomas of the breast are associated with clustered polymorphic microcalcifications.
3-screening lowers mortality most after age 50 and the dec is greater than that of a colonscopy or a pap smear
__________________________________________________________________
Now pharm
_____________
will start with infectious disease because it is the longest chunk
Acyclovir/valcyclovir/famiciclovir
all the above are the correct answer for
Herpes simplex including, genital, cutaneous, orolabial
for Herpes Encephalitis (acyclovir) IV form only in a hospital setting
Varicella zoster
shingles: Herpes zoster or reactivation
Bell's palsy
the above meds work by inhibition of thymidine kinase
-most common adverse effects are nephrotoxicity presumably from precipitation of the meds in the kidney tubule, sx of neurological toxicity in the kidney tubule, sx of neurological tox, such as confusion, tremors and hallucination occur rarely
____________________________________________________
Rifaximin
used to treat travelers' diarrhea such as that from E.coli, it isn't used for invasive diarrhea. an associated fever and bloody diarrhea indicate and invasive pathogen, such as campylobacter. When fever and bloody diarrhea are described, ciprofloxacin is the best answer.
rifa is a nonabsorbed version of the rifamycin antibiotic, it inhibits ribosomal RNA production of essential proteins
There are no major side effects since it isn't absorbed from the GI tract. it doesn't cause C.Diff, and may in fact treat it.
_________________________________________________
Daptomycin and Linezolid
they are both used for gram +ve organisms such as MRSA, streptococci and vanc resistant enterococci. Linezolid is the only oral antibiotic for MRSA. They can both be used for Vanc resistant organisms .
Liezolid is an oxazolidinone and inhibits protein synthesis at the ribosome. Daptomycin is a cyclic lipopeptide and disrupts cell membrane they are both unique classes of drugs
Linezolid commonly causes thrombocytopenia, and is a MAO inhibitor, avoid tyramine foods. Dapto caused CPK on liver functiion tests to be elevated!!
_______________________________________________________________
Tigecycline
an extremely broad spectrum anti-biotic that covrers MRSA, staph aureus, and well as gram negative bacilli. Tigecycline is the answer for complicated hospital of ICU acquired infections, tigecycline alone is equivalent to vanc and aztreonam in combination, it is also active against resistant enterococci and PCN resistant penumococcus
tigecycline is a glyclycyline antibiotic that binds to the ribosome and inhibits protein synthesis, it is unique that it covers staph, strep, gram negatives, anerobes and organisms resistant to vanc
tigecycline is hepatotoxic , caused nausea and diarrhea
__________________________________________________________
Polymyxin B (PMB) and colistin
useful for conjunctivitis, infections of the skin, and otitis externa, also correct for multi drug resistant gram negative bacilli, that cause ventilator associated pneumonia and sepsis from pseudomonas or acinetobacter.
works by disrupting phospholipids in the cell wall membrane
Polymyxin B (PMB) and colistin are very toxic to the kidney and nerves and is limited to topical applications of the skin and ear, they are also used for multi drug resistant gram negative bacilli when there are no other therapeutic options..
________________________________________________________
That is it for today..

In my pre-clinical years, I was president of the pharmacology club, and I enjoyed teaching it and exchanging ideas with others.. so if you have your own forte, quirks mnemonics that you'd like to share we can make a useful compendium..
I am only going to focus here on pharmacology and diagnostic testings.. so every day I'll give you five of each..
I am not going to start in any particular order but once in a section, I plan to complete it.. this will be just the high yield..
_____________________________________________________________
Oncology diagnostic testing
_____________
AFP (what disease is associated with it, and when do you answer this for a question?)
AFP is associated with the development of
1-hepatocellular ca.
2-ovarian cancer
3-non-seminomatous germ cell tumors
Answer AFP when you see a patient with alcoholic cirrhosis or chronic hepatitis B or V. AFP together with radiological imaging is used to screen for hepatocellular ca
____________________________________________
CEA
1-A protein elevated in a variety of cancers including colorectal cancer
2-serum CEA have a prognostic value in pts with newely diagnosed CRC. Those with higher levels have worse prognosis.
3-CEA level to monitor in colon cancer in pts after a surgical resection, it determines the presence of persistent, recurrent or metastatic disease
_____________________________________________________________
Colposcopy
Colposcopy is the direct visualization of the cervix, by use of a magnifying scope with a lamp
2-The transition zone must be visualized to ensure an adequate colposcopy. The border between squamous and columnar epithelium
3-a colposcopy is the answer for a pt with an abnromal pap
Atypical squams can't exclude high grade lesion ASC-II
low grade squamous intraepithelial lesions LSIL
high grade intraepithelial lesions HSIL
Atypical sqams of undetermined significance ASCUS if HPV DNA testing is positive
_____________________________________________________________
Estrogen and progesterone receptors
Should be done on all pts with breast cancer, in order to determine who should receive hormone therapy
2-Therapy with either tamoxifen or raloxifene should be added to any pt. with positive receptors. This is either for estrogen or progesterone positivity alone or in combination. The response to tamoxifen is better if both receptors are positive
______________________________________________________
Mammogram
screening should begin at age 40 and should be performed every 1~2 years, screening at age 50 should be yearly
2-when mammogram shows abnormalities, a core biopsy including sentinel lymph node biopsy is the next best step. carcinomas of the breast are associated with clustered polymorphic microcalcifications.
3-screening lowers mortality most after age 50 and the dec is greater than that of a colonscopy or a pap smear
__________________________________________________________________
Now pharm
_____________
will start with infectious disease because it is the longest chunk
Acyclovir/valcyclovir/famiciclovir
all the above are the correct answer for
Herpes simplex including, genital, cutaneous, orolabial
for Herpes Encephalitis (acyclovir) IV form only in a hospital setting
Varicella zoster
shingles: Herpes zoster or reactivation
Bell's palsy
the above meds work by inhibition of thymidine kinase
-most common adverse effects are nephrotoxicity presumably from precipitation of the meds in the kidney tubule, sx of neurological toxicity in the kidney tubule, sx of neurological tox, such as confusion, tremors and hallucination occur rarely
____________________________________________________
Rifaximin
used to treat travelers' diarrhea such as that from E.coli, it isn't used for invasive diarrhea. an associated fever and bloody diarrhea indicate and invasive pathogen, such as campylobacter. When fever and bloody diarrhea are described, ciprofloxacin is the best answer.
rifa is a nonabsorbed version of the rifamycin antibiotic, it inhibits ribosomal RNA production of essential proteins
There are no major side effects since it isn't absorbed from the GI tract. it doesn't cause C.Diff, and may in fact treat it.
_________________________________________________
Daptomycin and Linezolid
they are both used for gram +ve organisms such as MRSA, streptococci and vanc resistant enterococci. Linezolid is the only oral antibiotic for MRSA. They can both be used for Vanc resistant organisms .
Liezolid is an oxazolidinone and inhibits protein synthesis at the ribosome. Daptomycin is a cyclic lipopeptide and disrupts cell membrane they are both unique classes of drugs
Linezolid commonly causes thrombocytopenia, and is a MAO inhibitor, avoid tyramine foods. Dapto caused CPK on liver functiion tests to be elevated!!
_______________________________________________________________
Tigecycline
an extremely broad spectrum anti-biotic that covrers MRSA, staph aureus, and well as gram negative bacilli. Tigecycline is the answer for complicated hospital of ICU acquired infections, tigecycline alone is equivalent to vanc and aztreonam in combination, it is also active against resistant enterococci and PCN resistant penumococcus
tigecycline is a glyclycyline antibiotic that binds to the ribosome and inhibits protein synthesis, it is unique that it covers staph, strep, gram negatives, anerobes and organisms resistant to vanc
tigecycline is hepatotoxic , caused nausea and diarrhea
__________________________________________________________
Polymyxin B (PMB) and colistin
useful for conjunctivitis, infections of the skin, and otitis externa, also correct for multi drug resistant gram negative bacilli, that cause ventilator associated pneumonia and sepsis from pseudomonas or acinetobacter.
works by disrupting phospholipids in the cell wall membrane
Polymyxin B (PMB) and colistin are very toxic to the kidney and nerves and is limited to topical applications of the skin and ear, they are also used for multi drug resistant gram negative bacilli when there are no other therapeutic options..
________________________________________________________
That is it for today..




















.jpg)







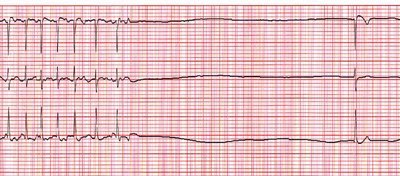
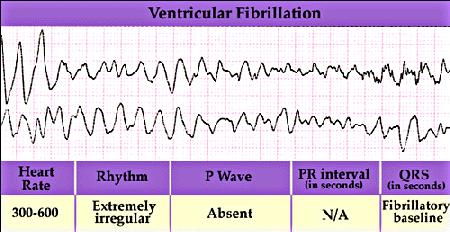
 .. just checking to see if you are reading lol
.. just checking to see if you are reading lol
